AI in Electronic Health Records 2026: Epic, Oracle Cerner, Athena
EHR AI in 2026 — Epic + GPT, Oracle Cerner Clinical AI Agent, Athena, Doximity GPT, Meditech Expanse AI. Problem-list summarization, inbox triage, FHIR + AI.

A primary-care physician at a US academic medical centre opens her Epic Haiku iPad before the first patient of the day. The in-basket has thirty-eight messages overnight. The AI in-basket panel has draft responses ready for twenty-nine of them — refill requests, normal-result notifications, simple follow-up questions. She reviews and sends most of them in twenty minutes between patients. Three years ago this was an hour of after-hours work; the in-basket was the single largest driver of provider burnout in the published literature. The shift happened quietly because the AI sits inside the workflow, not beside it.
The 2024–2026 wave of EHR-embedded generative AI is the most operationally consequential AI deployment in healthcare. It is not in the FDA-cleared-device tally because most of it sits outside the device regulatory perimeter, but it touches more clinicians per day than any imaging AI, drug-discovery platform, or telehealth tool. This post walks through the major EHR vendors’ AI surfaces, the FHIR-plus-AI architectural pattern that is emerging, the operational realities, and where the durable wins are.
The Epic generative-AI story#
Epic’s partnership with Microsoft and the OpenAI-derived models — first announced in 2023 — has shipped through the 2024–2026 release cycles into one of the most consequential AI surfaces in healthcare.
The headline features:
In Basket Augmented Response. AI generates draft replies to patient portal messages, scoped to the patient’s chart context. Adoption is broad; provider acceptance rates of the drafts vary by message type and specialty but cluster around half to two-thirds for routine messages. The bigger story is reduced after-hours work, with multiple published studies documenting the effect.
Chart Summary. AI summarisation of the patient chart for pre-visit preparation, hand-off, and consult contexts. The “Look-back” feature surfaces a contextual narrative across an extensive longitudinal record.
Note Templates with AI Assist. Auto-population of structured note sections, problem-list reconciliation, after-visit summary generation.
Chart Search Natural Language Queries. Ask “when was her last colonoscopy?” or “what statin has he failed?” — semantic search over the chart.
Showroom Integrations. Deep integration paths for ambient-scribe vendors (Abridge, DAX Copilot, Suki, others) into the documentation workflow.
The combined effect at a typical large Epic site by 2026: a clinician’s in-EHR experience has generative AI threaded through the documentation, communication, and chart-navigation surfaces simultaneously. The aggregate productivity gain is meaningful and the burnout data is consistently positive.
Oracle Cerner — now Oracle Health#
Oracle’s Clinical AI Agent and the broader Oracle Health AI suite shipped through 2024–2026 with a feature surface broadly comparable to Epic’s. The Larry Ellison-personally-driven AI agenda accelerated the roadmap; the execution and integration depth remained a topic of debate in the deployed-customer community. The 2024 partnerships with NVIDIA for inference infrastructure and the embedded-Oracle-database-native vector capabilities gave the platform a differentiated infrastructure story.
The honest deployed-customer picture in 2026 is mixed but improving — large health systems on Cerner Millennium and Oracle Health are seeing meaningful AI feature rollouts, with the integration depth and stability varying by site.

Athena, Meditech, eClinicalWorks, and the mid-market#
Athenahealth anchored a strong cloud-EHR position in ambulatory and small-hospital markets. Their AI surfaces span documentation assistance, claims and coding automation, and a clinician-facing assistant that competes with the ambient-scribe layer.
Meditech Expanse Genius — Meditech’s generative-AI overlay on Expanse — shipped a chart-summary, ambient-scribe, and inbox-draft feature surface through 2025–2026.
eClinicalWorks built sumo (their AI offering) covering documentation, scribe, and patient-engagement use cases.
NextGen, Greenway, AdvancedMD ship varying AI features for their ambulatory bases.
Allscripts/Veradigm has had a more disjointed AI story across their multiple EHR platforms.
The mid-market and ambulatory EHR landscape is the second-largest AI deployment surface in healthcare by clinician count, even though it gets less coverage than the Epic-Cerner story.
The third-party AI overlay layer#
Outside the EHR vendor surfaces, a meaningful third-party layer has emerged:
Doximity GPT — the clinician-network’s AI assistant — offers HIPAA-compliant generative AI for routine documentation, letters of medical necessity, patient-friendly explanations, and chart-style queries. The clinician-network distribution channel is the strategic advantage.
Notable Health sits on top of EHRs with workflow automation across intake, referrals, prior auth, and clinical-summary surfaces.
Suki, Abridge, DAX Copilot, DeepScribe, Augmedix, Nabla, Ambience are the ambient-scribe layer (covered in the hospital-operations post) that integrates with EHR documentation workflows.
Glass Health built a structured clinical-reasoning AI tool aimed at residents and primary-care providers.
OpenEvidence, Pathway, UpToDate AI are the AI-augmented clinical reference platforms.
The FHIR-plus-AI architectural pattern#
The 2024–2026 maturation of HL7 FHIR R4 and the US Core data-set requirements created the substrate for the EHR-AI integration pattern. The pattern is now established:
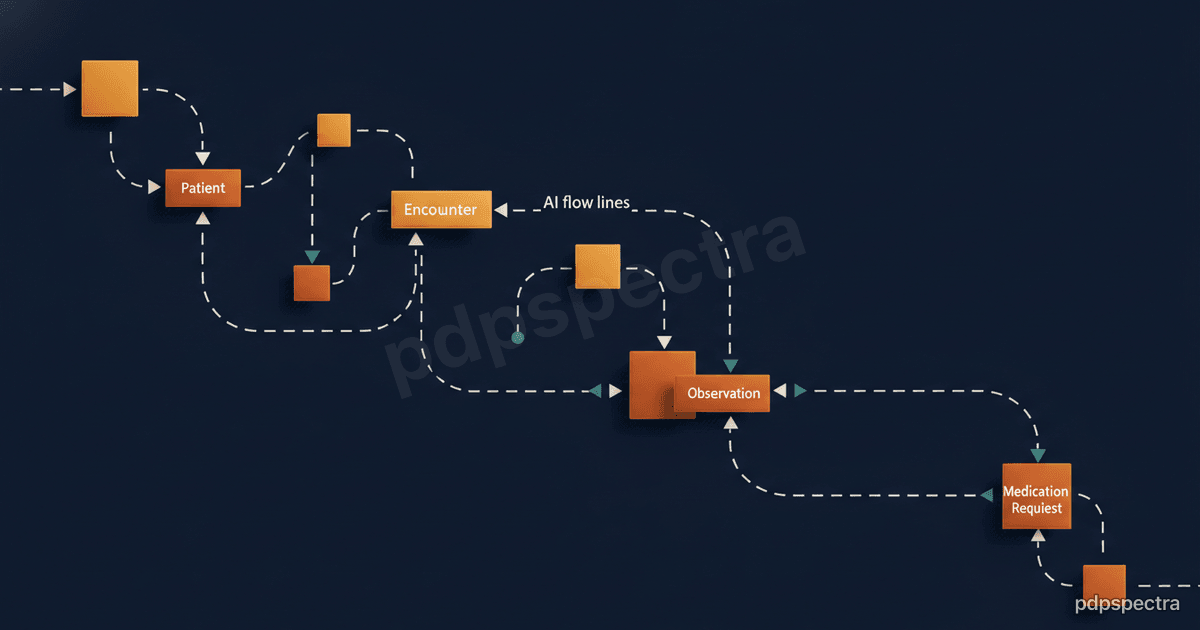
A FHIR API exposes the patient’s chart context (Patient, Encounter, Condition, MedicationStatement, Observation, DocumentReference). A SMART-on-FHIR launch context carries identity and authorization. The AI vendor’s service consumes the FHIR resources, runs the model, and writes results back via FHIR (Communication for inbox drafts, DocumentReference for notes, or proprietary write-back channels for EHR-specific surfaces). Audit logging flows through the EHR’s existing audit infrastructure or a parallel vendor-side audit log.
The Office of the National Coordinator’s USCDI versions, the TEFCA-anchored health-information-exchange substrate, and the CMS Patient Access and Interoperability rules pushed every major EHR vendor to expose meaningful FHIR APIs by 2024–2025. AI vendors that built against those APIs gained a portable integration pattern across multiple EHRs; vendors that built proprietary EHR integrations remain tightly coupled to specific platforms.
The use cases that actually pay back#
The honest 2026 read on EHR-AI ROI is clearer than three years ago.
Inbox triage and draft replies. Strong ROI, broad adoption, durable provider satisfaction. The single biggest operational win.
Ambient scribing. Strong ROI for ambulatory primary care and specialties with conversational visits; weaker fit for procedural specialties.
Chart summarisation for pre-visit and hand-off. Useful, broadly liked, but the productivity gain is harder to measure than the documentation use cases.
Problem-list reconciliation. Genuinely useful operationally but creates downstream coding and quality-measure implications that need careful governance.
Coding and claims automation. Mature, well-deployed, with the vendors split between EHR-native (Epic, Cerner) and specialised (3M 360, Optum, Codametrix). The risk profile around upcoding and audit exposure means clinical leadership has to set the guardrails.
Predictive risk surfaces (sepsis, deterioration, readmission). Mixed results in the deployed-evidence base. The early Epic Sepsis Model controversy (the 2021 JAMA evaluation showing meaningful under-performance versus the marketed claim) has been followed by a more cautious deployment posture. Several health systems now build their own predictive models against their own data.
Governance, audit, and the model-risk question#
Health systems running EHR-embedded AI at scale by 2026 have built — or are scrambling to build — model-risk governance that mirrors the financial-services model-risk-management framework. The components: a model registry covering every deployed AI surface, validation evidence for each, ongoing performance monitoring against site-specific data, a documented change-management workflow, a clinical-governance committee that signs off on deployment scope, and an incident-response procedure when a model misfires.
The HHS AI Procurement Guidance, the ONC Health Data, Technology, and Interoperability rules requiring AI transparency disclosures, and several state-level AI-in-healthcare laws (California, Texas, New York) push this from voluntary best-practice toward regulatory expectation.
Where pdpspectra fits#
We help health systems and EHR-adjacent vendors build the operational backbone around EHR-embedded AI — FHIR integration, model registries, validation pipelines, audit and observability, and the governance scaffolding that turns the rollout into a durable programme rather than a series of vendor pilots. See our AI and LLM integration practice.
Related reading#
- Voice AI in clinical documentation
- Healthcare AI playbook: pilot to production
- Hospital data interoperability
If you are scoping an EHR-AI programme — across Epic, Oracle Cerner, Athena, Meditech, or the third-party overlay layer — and want a pragmatic read on prioritisation, integration cost, and governance, reach out.